This course is currently in development.
This comprehensive online self-study course, will educate physicians about the application of neuroimaging strategies in the clinically identified patient with Parkinsonian symptoms. Further, the course will provide insight into using a combination of scans to gain further insight and improve the differential diagnosis among the Parkinsonian syndromes. Current diagnostic strategies without neuroimaging are highly inaccurate.
The specificity of clinical diagnosis is considerably lower without the aid of imaging. Psychogenic or pharmacological tremor can be confused with parkinsons disease leading to unnecessary treatment. Secondly, the other Parkinsonian syndromes can initially look indistinguishable from IPD. For example, the degree of DAT loss can help to predict the likelihood of the patient’s response to pharmacological treatment. Dopaminergic denervation follows a gradient from dorso-posterior to ventro-anterior striatum. Early identification of patients can greatly affect treatment and outcome. While the current arsenal of medications for parkinsons disease remains small, one thing is clear, the incorrect diagnosis can lead to untoward side effects and the risk of exposure to life threatening adverse events – such as in the case of Lewy body dementia and antipsychotic medications.
Disclosures: Faculty member Dr. Theodore Henderson and Planning Committee member Dr. Steven Mottl have no relationships with commercial interests that would constitute a conflict of interest. Disclosures were also obtained from MD Training @home staff: Nothing to Disclose.
Additional Course Information
Over 59,000 new cases of Idiopathic Parkinson’s Disease (IPD) are diagnosed in America each year. At least as many new cases of Parkinsonian syndrome cases also are identified annually. PSP affects approximately 1 in 100,000 persons over the age of 60. Roughly 20,000 persons in the U.S. have PSP. Multiple-system atrophy (MSA) is a rare degenerative neurological disorder. MSA affects approximately 4.6 persons per 100,000. The rate in males is slightly higher than in females and the typical age of onset is the late 50’s to early 60’s. Dementia with Lewy bodies (DLB) is affects 1.3 million persons in the U.S. alone. It shares clinical features similar to Alzheimer’s disease (AD) and IPD.
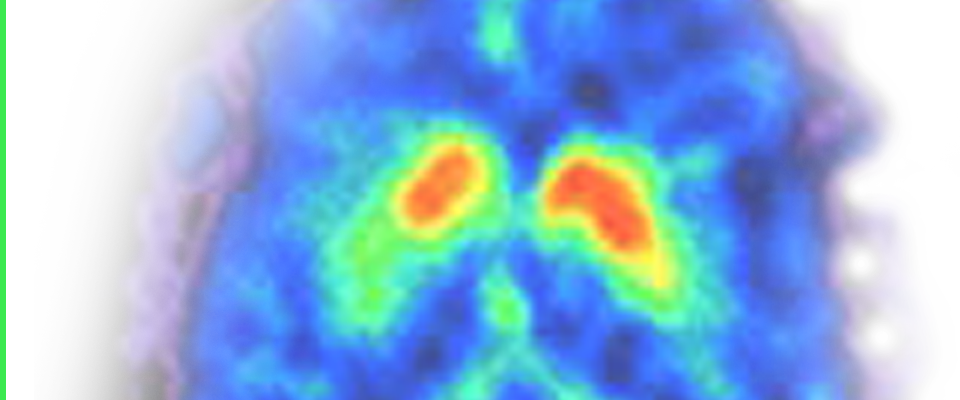
In 2011, I 123 Ioflupane became commercially available in the United States for imaging the dopaminergic system.It is marketed as DaTSCAN. The specificity of clinical diagnosis is considerably lower than DaTSCAN. Psychogenic or pharmacological tremor can be confused with Park dz leading to unnecessary treatment. Secondly, the other Parkinsonian syndromes can initially look indistinguishable from IPD. For example, the degree of DAT loss can help to predict the likelihood of the patient’s response to pharmacological treatment. Dopaminergic denervation follows a gradient from dorso-posterior to ventro-anterior striatum.
Dopaminergic studies such as the DaTSCAN available and FDA-approved here in the United States may help in clarifying the diagnosis of patients with symptoms suggestive of PD. This includes those with essential tremor, vascular dementia, pharmacologically induced tremor. This can prevent misdiagnosis and the administration of medications which may have adverse effects.
Nigrostriatal denervation is not specific for PD and has also been demonstrated in patients with other Parkinsonian syndromes, such as multiple system atrophy, progressive supranuclear palsy, and dementia with Lewy Bodies. Combined presynaptic dopaminergic studies and perfusion or metabolic studies may aid in the distinction between early IPD and an atypical parkinsonian syndrome, Dementia with Lewy Bodies, or pharmacological parkinsonian symptoms.
Presynaptic DA imaging may help distinguish Dementia with Lewy bodies from prototypical Alzheimer’s Disease but not necessarily from IPD. Again, perfusion SPECT or FDG PET may help immensely in clarifiying the diagnosis.
Early identification of patients can greatly affect treatment and outcome. While the current arsenal of medications for park dz remains small, one thing is clear, the incorrect diagnosis can lead to untoward side effects and the risk of exposure to life threatening adverse events – such as in the case of Lewy body dementia and antipsychotic medications.
President and Chief Medical Officer at The Synaptic Space
Private practice as a Child, Adolescent and General Psychiatrist.
Board Certified in Psychiatry, Dr. Henderson brings a unique blend of expertise in neuroimaging, psychopharmacology and neurobiology.